Cornea
Rethinking Aberrations: the Low-Degree/High-Degree (LD/HD) Scheme
In this first part of a three-part series, surgeons will gain a renewed clinical understanding of aberrations.

Soosan Jacob
Published: Sunday, March 1, 2026
“ The way ophthalmologists usually describe ocular aberrations may actually be misleading—especially in complex corneas and post-refractive surgery eyes. “
Ophthalmologists now receive wavefront information in daily practice, whether from aberrometers, tomographers, or laser platforms. Nearly all these devices describe the ocular wavefront using Zernike polynomials, which have become the default ‘language’ of optical aberrations. However, the way Zernike polynomials are constructed can quietly distort what matters most clinically: the subjective sphero-cylindrical refraction and the quality of the retinal image. Some higher-order Zernike modes contain small but meaningful amounts of low-degree terms such as tilt and defocus. When higher-order aberrations (HOA) are large, this mixing can create confusing results: e.g., predict spurious myopia after refractive surgery and retinal image simulations that look worse than what the patient really sees.
The Gatinel–Malet (GM) decomposition, also called the Low-Degree/High-Degree (LD/HD) scheme, was developed to solve this problem. Rather than abandoning Zernike polynomials, it reorganises the terms of the wavefront expansion to enforce a strict separation:
· a low-degree (LD) component that contains all piston, tilt, defocus, and primary astigmatism and is sealed or ‘watertight’ and corresponds more faithfully to the subjective sphero-cylindrical refraction;
· a high-degree (HD) component completely free of any low-degree terms and which provides a more accurate prediction of the retinal image and visual quality derived from higher-order aberrations.
With this rearrangement, the functional relationship between the two domains becomes clearer: the LD part of the wavefront aligns better with subjective refraction, and the HD part predicts the retinal point spread function and visual quality more faithfully. The measured wavefront remains unchanged, but its contents are redistributed to better interpret aberrometry and match how clinicians think about refraction versus HOAs.
In this first part of a three-part series, Soosan Jacob speaks with Damien Gatinel MD, PhD, head of the Anterior and Refractive Surgery Department, Rothschild Foundation, Paris, France, to get a renewed understanding of wavefronts in clinical terms and discover why the way ophthalmologists usually describe ocular aberrations may actually be misleading—especially in complex corneas and post-refractive surgery eyes.
SJ: Professor Gatinel, most of us see Zernike polynomials every day on our aberrometers, but we don’t really think about the mathematics behind them. To set the stage, could you briefly remind us what a ‘wavefront’ is in clinical terms?
DG: Of course. In clinical optics, the wavefront describes the surface of an equal optical phase emerging from the eye. If that surface is perfectly flat across the pupil, all the emerging rays are parallel and focus on the retina—that’s emmetropia. If, instead, the wavefront assumes the form of a simple paraboloid of revolution—mathematically represented as a pure r² term—the eye is said to be defocused. A myopic wavefront is a convex (forward-bowed) paraboloid, whereas a hyperopic eye has a concave (backward-bowed) paraboloid. This type of defocus is classified as a low-degree aberration and can be completely corrected using ordinary spectacles or contact lenses.
Could you walk us through in some more detail about wavefronts and rays and why they matter clinically?
First, we often use light rays as a convenient way to visualise the local direction of light propagation. They are an abstraction, but a very useful one in clinical practice. In contrast, the wavefront represents the surface on which the optical phase is identical everywhere. So, while rays tell us which way the light is going, the wavefront tells us where the light is in its phase.
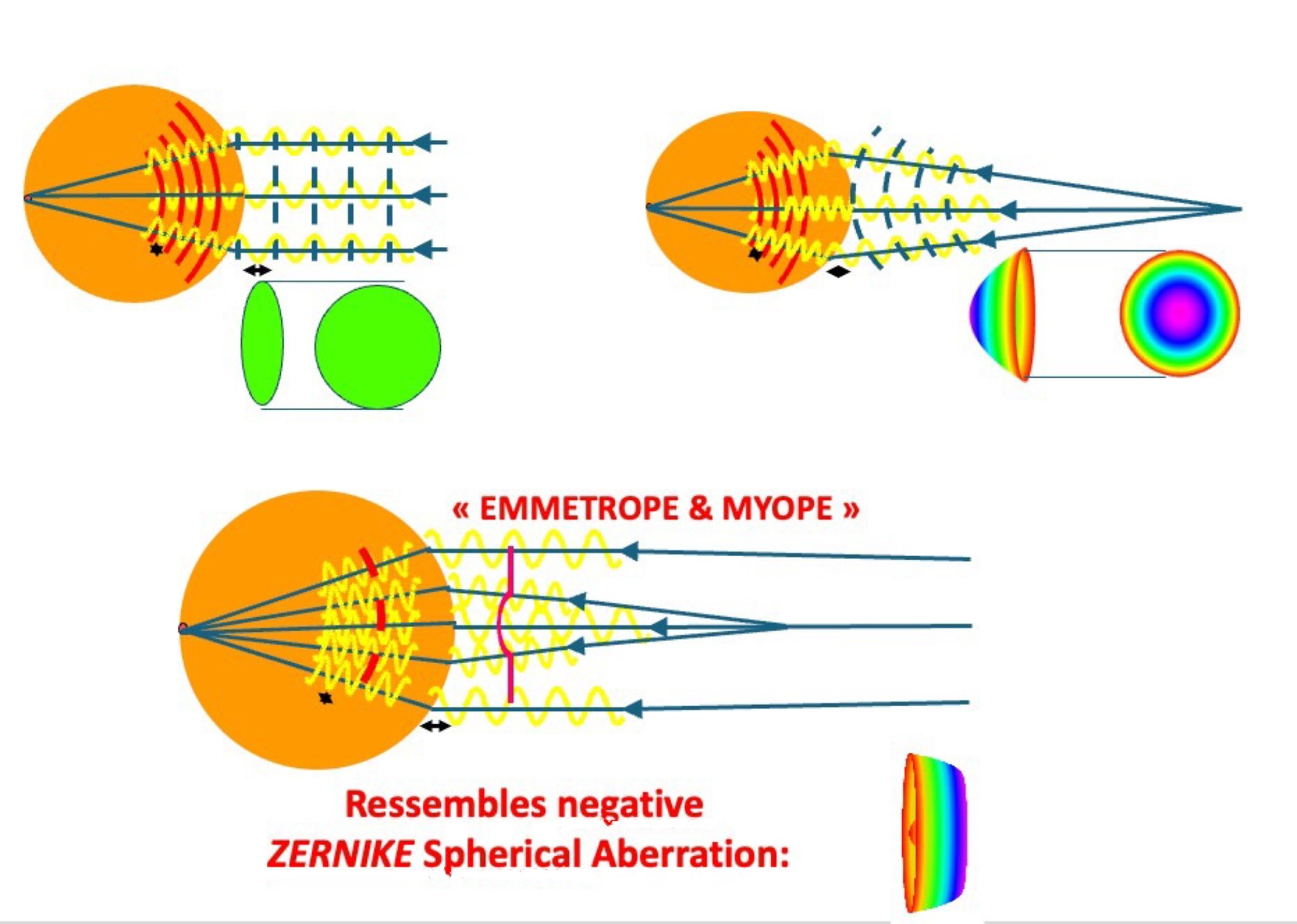
For clinicians, the most intuitive representation is often a map of vergence, like the one shown in the figure. This type of map tends to be the easiest to interpret clinically, as it directly relates to the convergence or divergence of the light at each point. Geometrically, the important point is that rays are always perpendicular to the wavefront at every location. You can think of rays as the trajectories photons would follow, orthogonal to that phase surface.
Looking at the figure reminds us how optical systems form images. They do this by refracting light as it passes through media with different refractive indices. When light enters a denser medium, its wavelength becomes shorter, but the frequency stays the same. If you count how many wavelengths fit along the path from the source to the image plane, you obtain the optical path length, which is exactly the total number of wavelengths between those two points. When this optical distance is identical for every ray travelling through the system, the resulting image is optically ‘perfect’: all contributions arrive in phase, and you get maximal constructive interference on the image plane.
In an emmetropic eye, an incident plane wavefront (light coming from infinity, for example) is transformed by the eye’s optics into a spherical wavefront that comes to focus on the fovea. In a myopic eye, the geometry is different. The wavefront that emerges from the retina is still spherical, but its centre of curvature lies at a finite distance in space; this point is the punctum remotum, or far point, of the myopic eye.
Finally, the bottom schematic in the figure shows how a negative Zernike spherical aberration behaves. Its shape mimics a multifocal wavefront. The central part of the wavefront is steeper and provides a focus for near vision, while the peripheral part is flatter, favouring distance vision. This multifocal-like profile is exactly why negative spherical aberration has been exploited in various presbyopia-correcting approaches, and the figure gives a visual intuition for that behaviour.
We’ve talked about defocus as a low-degree aberration that we can correct with glasses or contact lenses. What happens when we move to higher-degree terms—those we usually call higher-order aberrations?
That’s where things get interesting. Once the radial exponent of the wavefront term reaches 3 or higher, we are dealing with higher-degree aberrations, and these cannot be corrected through ordinary lenses. In practice, the most clinically relevant of these are the third-degree terms, which correspond to coma, and the fourth-degree terms, where spherical aberration is the key player. Ideally, when we talk about the ‘high-degree’ group, it should contain only genuine higher-degree terms—things that really start at r³, r⁴, and so on, without any hidden low-order content. However, some of the Zernike modes we routinely use violate this principle. A classic example is the Zernike spherical aberration mode (Z₀⁴). Mathematically, it is not a ‘pure’ r⁴ term; it actually contains a hidden quadratic (r²) component of defocus.
This shows up very clearly if you look at its shape. Instead of being a simple, uniformly concave or convex bowl with a relatively flat central portion—what you would expect from a pure r⁴ profile—the Zernike spherical aberration mode has a ‘sombrero-like’ appearance with a central inflection. That central steepening is exactly the signature of the embedded r² content. Visually, this morphology is reminiscent of a schematic multifocal wavefront: it is steeper and more parabolic in the centre, which favours near vision, and becomes flatter toward the periphery, which favours distance vision. This resemblance is not just an academic curiosity; it helps explain why the negative spherical aberration profile of the Zernike mode has been historically popular in presbyopia-correcting strategies. Both corneal photoablations and refractive simultaneous vision intraocular lenses have often been designed around this type of profile, precisely because it mimics a multifocal behaviour at the level of the wavefront.
And that’s where Zernike polynomials come in?
Absolutely! Zernike can mislead when HOAs are large. Zernike polynomials (Zm) are mathematically sophisticated functions that constitute a complete, orthogonal set over a circular pupil. In practical terms, this implies that, from a purely mathematical point of view, each mode is independent of all the others, and the total wavefront error can be written as the quadratic sum of the individual coefficients, in accordance with the Pythagorean principle. Because of this orthogonality, we can calculate a single global root mean square (RMS) value and combine the contributions of all low- and high-degree modes without any overlap between them.
In the physical sciences—where Zernike polynomials were originally introduced—this kind of global orthogonality is crucial. It guarantees that each mode has a unique contribution to the overall optical error, and there is no distinction between aberrations that can be corrected with spectacles and those that cannot. In ophthalmology, however, this same feature leads to a subtle paradox. To preserve strict orthogonality across the full set of polynomials, certain higher-order Zernike modes are forced to contain small amounts of lower-order terms. For example, the Zernike coma modes (Z3±1) include a linear component (r1, corresponding to tilt), and the spherical aberration modes (Z40, Z60) incorporate a quadratic component (r2, corresponding to defocus). These embedded lower-order pieces are what keep the basis rigorously orthogonal, but they do so at the expense of clinical interpretability.
You’ve explained that some Zernike modes ‘mix’ true higher-order content with hidden low-order components like defocus or astigmatism. Clinically, what problems does this mixing create, and how does the LD/HD approach help us get around them?
In practical terms, this structural mixing has at least three important consequences for us as clinicians. First, a portion of the low-degree information—defocus or regular astigmatism—can be buried inside the higher-order modes. As a result, the low-degree Zernike coefficients that we usually rely on become unreliable predictors of the true sphero-cylindrical refraction. Second, because some low-degree curvature is embedded within the high-degree modes, retinal image simulations based on the Zernike expansion can look worse than the patient’s real-life vision. This discrepancy is especially striking when there are large higher-order aberrations: the simulated point-spread function or retinal image may appear excessively degraded, even though the patient’s subjective experience is better once refraction is optimally corrected. Third, there is a reciprocal effect: the numerical amplitudes of the high-degree Zernike coefficients are artificially lowered. Their coefficients appear deceptively small, even though their true contribution to wavefront deformation remains substantial.
From an ophthalmic standpoint, we really need a different kind of separation. Ideally, the low-degree modes should describe the curvature of the wavefront near the centre of the pupil—the region that determines the sphero-cylindrical refraction. The high-degree modes, by contrast, should capture the deformations that develop toward the pupil periphery, while staying as flat and neutral as possible in the central zone.
This is exactly the type of strict separation that the Gatinel–Malet (LD/HD) decomposition provides. In the accompanying figure, we illustrate this by converting the Zernike spherical aberration mode (Z₄⁰) with a negative coefficient into dioptres. The result shows that this mode is far from refractively neutral: its central curvature behaves as if it contains a significant amount of defocus, even though we tend to think of spherical aberration as a purely higher-order effect.
This conversation will be continued in the next issue of EuroTimes.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.