What are the benefits and techniques for performing thin-flap LASIK? Cheryl Guttman Krader reports.
Cheryl Guttman Krader
Published: Tuesday, March 1, 2022
What are the benefits and techniques for performing thin-flap LASIK? Cheryl Guttman Krader reports.
Photorefractive keratectomy was the initially recommended method for retreatment after SMILE. Alternatively, refractive surgeons can choose from two other approved “on-label” procedures that involve converting the SMILE cap into a LASIK flap either by the CIRCLE technique or with a side cut only.
For Dan Z Reinstein MD, MA (Cantab), FRCSC, FRCOphth, DABO, FEBO, however, an off-label thin-flap LASIK technique is the preferred approach.
“LASIK is a great procedure that gives patients the fastest visual recovery in a way that, for [their] experience, is also the least invasive. It has the best accuracy and, compared to the CIRCLE or sidecut only procedure, thin-flap LASIK preserves a greater amount of uncut stroma,” he said.
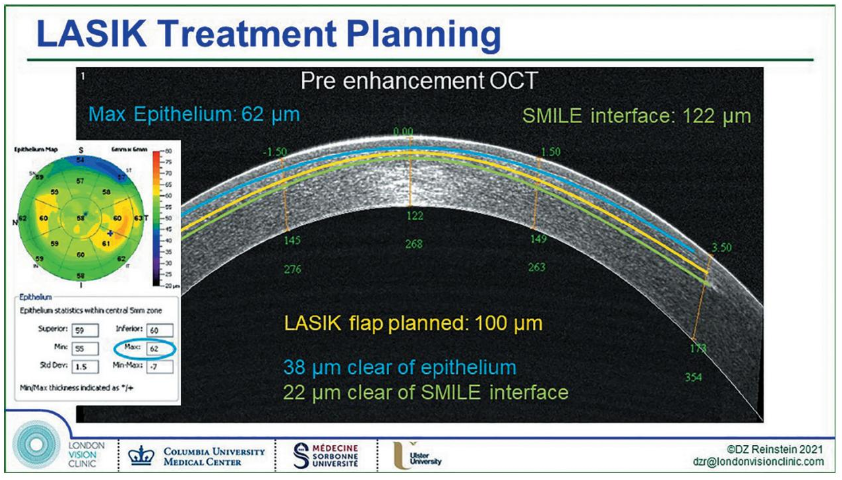
PLANNING FLAP THICKNESS
Dr Reinstein said he generally performs SMILE with a minimum of a 135 μm cap because this has the benefit of maximising corneal nerve preservation and biomechanical residual strength.i Additionally, using a 135 μm cap almost always allows for a thinflap LASIK enhancement with a 100 μm flap. Surgeons in the US who must do SMILE with a 120 μm cap can create a 90 μm flap when doing a LASIK retreatment, he suggested.
The flap thicknesses he recommended for these two scenarios mathematically derive from calculations that consider the standard deviation of the VisuMax femtosecond laser and the creation of a flap that will not cross superficially into the epithelium or deeper into the SMILE interface. As an added precaution, Dr Reinstein routinely evaluates epithelial and cap thicknesses on a three-dimensional pachymetry map obtained using the very high-frequency digital ultrasound Insight® 100 (ArcScan Inc) or an anterior segment optical coherence tomography such as the MS-39 (CSO Italia) to assess the three-dimensional biometry, and hence safety of performing a thin-flap LASIK enhancement.
LESSONS FROM THE LEARNING CURVE
The safety and success of performing a thin-flap LASIK enhancement over SMILE also involve the use of a specific flap lift technique and appropriate LASIK nomogram.
“We now teach the specifics of LASIK over SMILE in our Forefront Refractive Surgery Courseii and have delineated the method in our textbookiii so others may learn from all of the difficulties we encountered during the development of this protocol,” Dr Reinstein said.
The flap lift technique Dr Reinstein developed at the London Vision Clinic was refined over time to minimise the risk of tearing the SMILE incision or entering the SMILE interface, creating multiple planes. Described as a bimanual inferior pseudo-hinge fulcrum technique, a review of outcomes for a total of 135 LASIK retreatment cases performed using different flap lift techniques established its safety.iv The analysis, updated to include all treatments to date, showed no complications occurred in the last 237 retreatments, which represented all cases performed using the optimised approach.
Dr Reinstein said analyses of the refractive outcomes of the LASIK enhancements showed good accuracy for correcting astigmatism and hyperopia.v However, the analyses did note a tendency for overcorrection in cases of myopic enhancements. He explained that, in retrospect, this could have been expected, as he performed these myopic enhancements using the same nomogram as for consecutive myopic LASIK enhancement. The epithelial profile changes after myopic SMILE being different from those of LASIK require a different nomogram. The analysis found no nomogram adjustment was needed for enhancements after SMILE using the TSA or Triple-A ablation profiles on the MEL 90 – although the data entry did need to be increased for enhancements after LASIK.
This presentation was made at the 39th Congress of the ESCRS in Amsterdam.
i Reinstein DZ, Archer TJ, Randleman JB. “Mathematical model to compare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction”. Journal of Refractive Surgery. 2013 Jul; 29(7): 454–460. doi: 10.3928/1081597X-20130617-03. Erratum in: Journal of Refractive Surgery. 2017 Nov 1; 33(11): 788. PMID: 23820227.
ii www.londonvisionclinic.com/courses
iii The Surgeon’s Guide to SMILE. Reinstein DZ, Archer TJ, Carp GI. ISBN 10: 1630912654. Slack Inc. 2018.
iv Journal of Cataract & Refractive Surgery. 2018; 44(11): 1355–1362.
v Reinstein DZ, Carp GI, Archer TJ, Vida RS. “Outcomes of Retreatment by LASIK after SMILE”. Journal of Refractive Surgery. 2018 Sept 1; 34(9): 578–588. doi: 10.3928/1081597X-20180717-02. PMID: 30199561.
Dan Z Reinstein MD, MA (Cantab), FRCSC, FRCOphth, DABO, FEBO is the medical director of the London Vision Clinic, London, UK.
dzr@londonvisionclinic.com