Errant rhexis
There are ways to master the complication of a disobeying rhexis in phacoemulsification

Soosan Jacob
Published: Friday, March 1, 2019
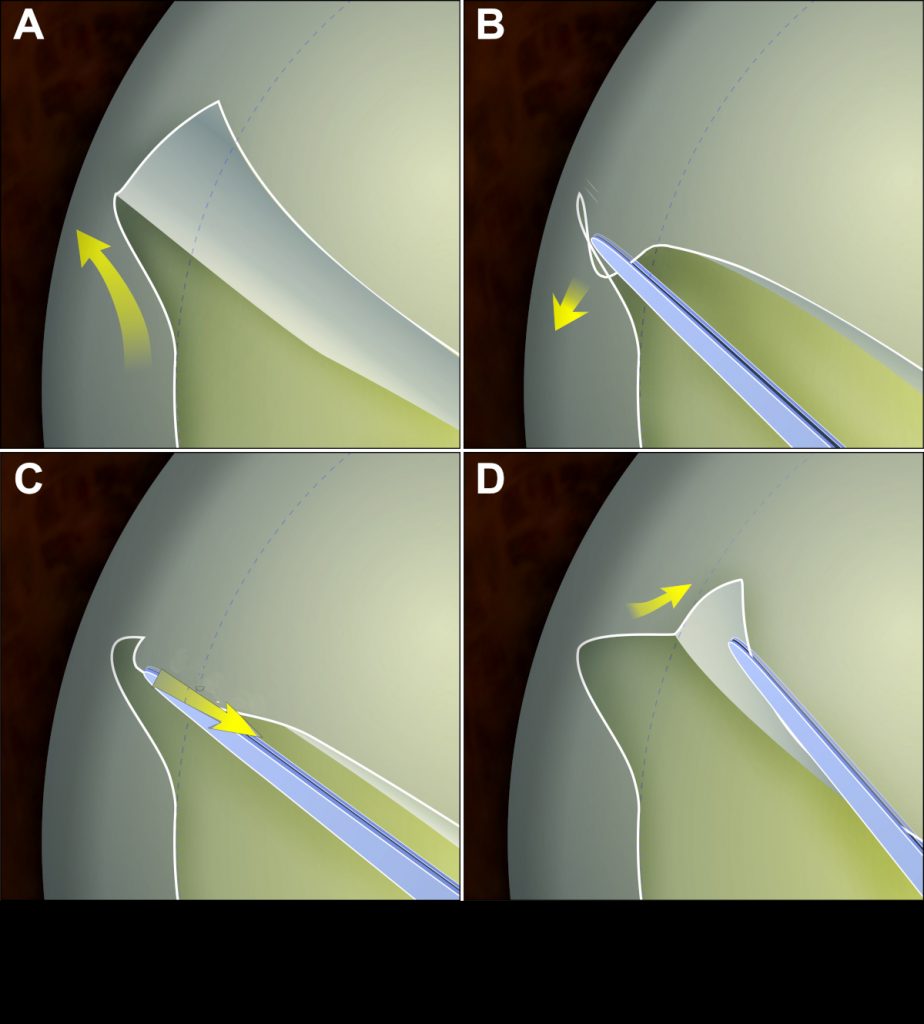 The Little rhexis trick in four steps. A: Peripheral extension. B: Capsular flap unfolded to lie flat. Holding the flap as close to the root as possible, it is first pulled backwards in a horizontal plane along the circumference of the completed segment of rhexis. C: With flap held stretched, force is directed more centrally to bring the rhexis back in. D: The rhexis is then continued again[/caption]
A continuous, perfectly circular, sized and centred rhexis is the all-desirable step in phacoemulsification – stretching comfortably for phaco manoeuvres without wrap-arounds and overlapping the IOL optic 360 degrees around, thus preventing posterior capsular opacification, delayed asymmetric capsular shrinkage, pea-podding of haptic, IOL vaulting or decentration, optic edge capture or IOL position/ refraction changes.
Increasing surgeon experience, aids such as corneal rhexis markers, millimetre-marked rhexis forceps, image-guided overlay technologies as well as the femtosecond laser or the Zepto capsulotomy systems have further helped increase precision. Many of us, however, still mostly rely on a manual rhexis with either forceps or cystitome, and are sometimes faced with a disobeying rhexis. This article helps deals with this.
PEARLS FOR A GOOD RHEXIS
A flat anterior lens capsule and low intra-lenticular pressure help keep the rhexis on track. It is therefore important to have a soft eye, a patient who is not straining and lids that are not squeezing.
Beginners may be benefitted by a peribulbar block and a Pinkie ball or Honan balloon application. A self-retaining speculum helps decrease the effect of lid squeezing. Good topical anaesthesia and a dilated pupil make both surgeon and patient more comfortable.
Capsular dye (Trypan blue 0.06%) improves visualisation. A partial entry allows better retention of viscoelastic in the anterior chamber (AC) and can be widened later. An oblique bend to the cystitome tip allows it to be visualised as opposed to a right-angled bend. Shaft angulation should avoid incisional distortion secondary to excessive anterior or posterior pressure. Alternately, a microrhexis forceps may be used, which, as compared to Utrata forceps, requires only a tiny incision and therefore avoids escape of viscoelastic.
Whenever required, viscoelastic should be replenished to maintain a flat anterior capsule. The flap edge is released and regrasped close to the tearing edge for better control.
The initial nick should be just short of the desired radius as it enlarges slightly on turning circularly. The rhexis edge mirrors the curve of the capsular flap edge and maintaining the flap flat and circular against the lens gives a perfect circle. Turning the flap inwards or outwards can make the rhexis smaller or larger respectively.
Near the main port, avoid a floating flap from sliding out through the incision, which can lead to peripheral extension of rhexis. In an average-sized eye, a uniformly dilated pupil may be used as a guide for centration and sizing; however, this would be erroneous in large or small eyes.
FACTORS PREDISPOSING TO AN ERRANT RHEXIS
Shallow AC, convex anterior lens capsule, poor visualisation, small pupil, paediatric cataracts, traumatic cataract with anterior capsular tear, white mature or Morgagnian cataract are some of the reasons a rhexis may run out.
Young cataracts: Rhexis in a child or young adult has a higher tendency to run out because of an elastic capsule, positive vitreous pressure and low ocular rigidity. The younger the age, the stronger the run-out tendency. Trypan blue can aid visualisation as well as stiffen the capsule.
Aiming for a smaller size allows a final rhexis of the desired size as the elastic capsule stretches. The first nick should therefore be made smaller than in an adult cataract. The tear is always directed towards the centre of the lens to avoid a runaway. A high viscosity ophthalmic viscosurgical device (OVD) (Healon5 and Healon GV) may be used to maintain space and flatten the anterior capsule.
Various other techniques such as vitrectorhexis, two-incision push-pull technique, Fugo Blade rhexis etc have also been described. Depending on age, a posterior continuous curvilinear capsulorhexis (PCCC) may be required.
White cataracts: The capsule in a mature, white cataract is thin, with higher likelihood of tears and run-outs. Intra-lenticular pressure in in tumescent white cataract is quite high and the initial nick can extend rapidly to both sides resulting in the “Argentinian flag sign”. Risk factors include diabetes, UV exposure, steroid usage etc. Staining stiffens and makes the capsule brittle and may also be a risk factor. Oblique external illumination with a light pipe can help visualisation. An initial small rhexis can be spiralled around to the right size to prevent a runaway.
Morgagnian cataract: These leak and cloud the aqueous. Aspiration with a needle from the centre of the capsule before initiating the rhexis can decrease intra-lenticular pressure and leakage. In case of a turbid AC, it should be washed and high viscosity OVD refilled. Once lens material is released, intra-lenticular support for needle capsulorhexis may be inadequate and a forceps may be required to continue.
Difficult visualisation: Secondary to corneal opacity, mature cataract, a poor red glow because of vitreous haemorrhage/asteroid hyalosis or inadequate co-axial lighting. Visualisation can be enhanced by capsular staining, high magnification, co-axial lighting and oblique illumination with a light pipe.
RUNAWAY RHEXIS
Blind pulling is avoided to avoid posterior capsular extension. The Little rhexis trick, popularised by Brian C Little, is very useful (see illustration, above). The capsule flap is unfolded to lie flat. While holding it as close to the root of the tear as possible, it is first pulled backwards in a horizontal plane along the circumference of the completed segment of rhexis and then with flap held stretched, directed more centrally to initiate the tear. If the rhexis run-out is irretrievable, it may be attempted to be completed by creating a cut on the flap and continuing forwards or by creating a nick on the opposite side and completing it backwards.
Alternatively, can-opener cuts can be done in the incomplete area. For Argentinian flag sign, AC pressure should be immediately increased with cohesive OVD to prevent wraparound tear. A perpendicular relaxing cut on the leaflet is then joined on either side as a partial circular tear. Surgery should be as in torn rhexis.
TORN RHEXIS
Only a continuous curvilinear rhexis can stretch. Tensile strength of the capsule is lost in case of any discontinuity, however small. All intra-capsular manoeuvres should therefore be avoided and the nucleus prolapsed out. Very careful, slow-motion phaco is then carried out.
In case of doubt or lack of experience, it may be better to convert into an extracapsular cataract extraction.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
Update (12-03-2019): An earlier edition of this article referred to the "little rhexis". This was an editorial oversight. It is the Little rhexis technique, popularised by Brian C Little, UK.
The Little rhexis trick in four steps. A: Peripheral extension. B: Capsular flap unfolded to lie flat. Holding the flap as close to the root as possible, it is first pulled backwards in a horizontal plane along the circumference of the completed segment of rhexis. C: With flap held stretched, force is directed more centrally to bring the rhexis back in. D: The rhexis is then continued again[/caption]
A continuous, perfectly circular, sized and centred rhexis is the all-desirable step in phacoemulsification – stretching comfortably for phaco manoeuvres without wrap-arounds and overlapping the IOL optic 360 degrees around, thus preventing posterior capsular opacification, delayed asymmetric capsular shrinkage, pea-podding of haptic, IOL vaulting or decentration, optic edge capture or IOL position/ refraction changes.
Increasing surgeon experience, aids such as corneal rhexis markers, millimetre-marked rhexis forceps, image-guided overlay technologies as well as the femtosecond laser or the Zepto capsulotomy systems have further helped increase precision. Many of us, however, still mostly rely on a manual rhexis with either forceps or cystitome, and are sometimes faced with a disobeying rhexis. This article helps deals with this.
PEARLS FOR A GOOD RHEXIS
A flat anterior lens capsule and low intra-lenticular pressure help keep the rhexis on track. It is therefore important to have a soft eye, a patient who is not straining and lids that are not squeezing.
Beginners may be benefitted by a peribulbar block and a Pinkie ball or Honan balloon application. A self-retaining speculum helps decrease the effect of lid squeezing. Good topical anaesthesia and a dilated pupil make both surgeon and patient more comfortable.
Capsular dye (Trypan blue 0.06%) improves visualisation. A partial entry allows better retention of viscoelastic in the anterior chamber (AC) and can be widened later. An oblique bend to the cystitome tip allows it to be visualised as opposed to a right-angled bend. Shaft angulation should avoid incisional distortion secondary to excessive anterior or posterior pressure. Alternately, a microrhexis forceps may be used, which, as compared to Utrata forceps, requires only a tiny incision and therefore avoids escape of viscoelastic.
Whenever required, viscoelastic should be replenished to maintain a flat anterior capsule. The flap edge is released and regrasped close to the tearing edge for better control.
The initial nick should be just short of the desired radius as it enlarges slightly on turning circularly. The rhexis edge mirrors the curve of the capsular flap edge and maintaining the flap flat and circular against the lens gives a perfect circle. Turning the flap inwards or outwards can make the rhexis smaller or larger respectively.
Near the main port, avoid a floating flap from sliding out through the incision, which can lead to peripheral extension of rhexis. In an average-sized eye, a uniformly dilated pupil may be used as a guide for centration and sizing; however, this would be erroneous in large or small eyes.
FACTORS PREDISPOSING TO AN ERRANT RHEXIS
Shallow AC, convex anterior lens capsule, poor visualisation, small pupil, paediatric cataracts, traumatic cataract with anterior capsular tear, white mature or Morgagnian cataract are some of the reasons a rhexis may run out.
Young cataracts: Rhexis in a child or young adult has a higher tendency to run out because of an elastic capsule, positive vitreous pressure and low ocular rigidity. The younger the age, the stronger the run-out tendency. Trypan blue can aid visualisation as well as stiffen the capsule.
Aiming for a smaller size allows a final rhexis of the desired size as the elastic capsule stretches. The first nick should therefore be made smaller than in an adult cataract. The tear is always directed towards the centre of the lens to avoid a runaway. A high viscosity ophthalmic viscosurgical device (OVD) (Healon5 and Healon GV) may be used to maintain space and flatten the anterior capsule.
Various other techniques such as vitrectorhexis, two-incision push-pull technique, Fugo Blade rhexis etc have also been described. Depending on age, a posterior continuous curvilinear capsulorhexis (PCCC) may be required.
White cataracts: The capsule in a mature, white cataract is thin, with higher likelihood of tears and run-outs. Intra-lenticular pressure in in tumescent white cataract is quite high and the initial nick can extend rapidly to both sides resulting in the “Argentinian flag sign”. Risk factors include diabetes, UV exposure, steroid usage etc. Staining stiffens and makes the capsule brittle and may also be a risk factor. Oblique external illumination with a light pipe can help visualisation. An initial small rhexis can be spiralled around to the right size to prevent a runaway.
Morgagnian cataract: These leak and cloud the aqueous. Aspiration with a needle from the centre of the capsule before initiating the rhexis can decrease intra-lenticular pressure and leakage. In case of a turbid AC, it should be washed and high viscosity OVD refilled. Once lens material is released, intra-lenticular support for needle capsulorhexis may be inadequate and a forceps may be required to continue.
Difficult visualisation: Secondary to corneal opacity, mature cataract, a poor red glow because of vitreous haemorrhage/asteroid hyalosis or inadequate co-axial lighting. Visualisation can be enhanced by capsular staining, high magnification, co-axial lighting and oblique illumination with a light pipe.
RUNAWAY RHEXIS
Blind pulling is avoided to avoid posterior capsular extension. The Little rhexis trick, popularised by Brian C Little, is very useful (see illustration, above). The capsule flap is unfolded to lie flat. While holding it as close to the root of the tear as possible, it is first pulled backwards in a horizontal plane along the circumference of the completed segment of rhexis and then with flap held stretched, directed more centrally to initiate the tear. If the rhexis run-out is irretrievable, it may be attempted to be completed by creating a cut on the flap and continuing forwards or by creating a nick on the opposite side and completing it backwards.
Alternatively, can-opener cuts can be done in the incomplete area. For Argentinian flag sign, AC pressure should be immediately increased with cohesive OVD to prevent wraparound tear. A perpendicular relaxing cut on the leaflet is then joined on either side as a partial circular tear. Surgery should be as in torn rhexis.
TORN RHEXIS
Only a continuous curvilinear rhexis can stretch. Tensile strength of the capsule is lost in case of any discontinuity, however small. All intra-capsular manoeuvres should therefore be avoided and the nucleus prolapsed out. Very careful, slow-motion phaco is then carried out.
In case of doubt or lack of experience, it may be better to convert into an extracapsular cataract extraction.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
Update (12-03-2019): An earlier edition of this article referred to the "little rhexis". This was an editorial oversight. It is the Little rhexis technique, popularised by Brian C Little, UK.