
Deciding on the choice of IOL to implant can sometimes be a difficult task, not only for the patient but also often for the surgeon who counsels the patient. The numerous types of available IOLs as well as relative advantages and disadvantages of each can be daunting.
At the outset, before explaining the various types of IOLs available, it is wise to try and find out what activities matter most to the patient, how they feel about wearing glasses some/all of the time and to know if they want/ expect complete spectacle independence. This conversation helps in guiding patients towards the possible best choice for them as well as helps in setting realistic expectations preoperatively.
Questionnaires and informational videos can help set the stage for a one-on-one direct discussion with the patient.
Understanding the patient’s lifestyle and visual preferences – whether there is a requirement for greater clarity at distance, intermediate or near vision is important. It is also important to set realistic expectations regarding a reasonably but not completely glasses-free life, and clear understanding that some activities will need glasses.
It is generally advisable to focus on good distance visual acuity in the dominant eye and either have better intermediate or near vision in the non-dominant eye depending on the patient’s requirement.
Taller patients have a slightly farther requirement for their near point than shorter patients and the body build should also be considered. Possible need for postoperative laser vision correction for any residual refractive error should be kept in mind by the surgeon and informed to the patient. There should be preoperative clarity about the financial considerations for this possible enhancement.
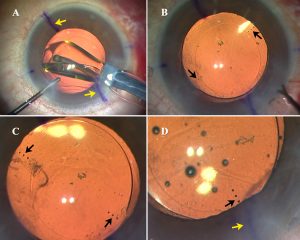
Fig A: Toric IOL seen being implanted. Alignment marks on cornea are visible (yellow arrows); B- IOL implanted in-the-bag. Alignment marks on IOL are visible (black arrows); C- IOL is rotated to lie short of the corneal alignment marks following which viscoelastic is completely removed; D- IOL is rotated into its final position.
STANDARD MONOFOCALS
I still use monofocal IOLs for many of my patients who do not want premium IOLs. Knowing their visual demands helps to plan better. Patients opting for monovision or micromonovision have the dominant eye focused for distance and the other for near/ intermediate by aiming for slight myopia. These patients should be given a monovision trial prior to surgery to check suitability and to get a first-hand preoperative experience of monovision.
PREMIUM IOLs
Before choosing a premium IOL, I always try to make sure the patient is a good candidate. A healthy ocular surface allows accurate IOL power calculations and a satisfied patient post-operatively. History, variable measurements and irregular patterns on topography and ocular staining are important and any dry eye is treated pre-operatively if present. A macular OCT helps rule out early maculopathy. I also look for large-angle kappa and increased higher-order aberrations, which may result in unhappiness with multifocal IOLs. Astigmatism on topography and keratometry help determine the need for toric or multifocal toric IOLs.
Multifocals: These IOLs use diffractive optics and split light into far and near foci, thereby creating peaks at individual focal points that the patient can focus on. However, blurry vision in between the two foci and glare and haloes from the other images are disadvantages.
I prefer implanting multifocals after a detailed conversation with the patient about the expected benefits as well as the visual symptoms that may occur, especially during night driving.
A mix-and-match policy can help expand the range of vision offered by different multifocals. Newer rotationally asymmetric segmented bifocal IOLs with sector-shaped near vision segment give far and near (+3D add) focus zones for better depth of focus and include the Mplus, Mplus X (Oculentis) and SBL-3 (Lenstec).
Trifocals – AT LISA (Carl Zeiss Meditec), FineVision (PhysIOL, Belgium), PanOptix (Alcon), Alsafit (Alsanza) and Acriva Reviol (VSY Biotech) – provide better intermediate vision with fewer side-effects. Most also have toric versions.
Extended Depth of Focus (EDOF) IOLs: I like EDOF IOLs because of the better intermediate vision they provide with lesser side-effects of glare, halos or loss of contrast as compared to multifocals. EDOFs would be preferred more than multifocal IOLs in maculopathy or irregular corneas, though monofocals would still be the first choice in these cases.
They have an elongated focal area, giving an extended depth of focus, minimal effect on peak resolution and give reasonably clear vision at all distances (especially far and intermediate). However, near vision with a higher add multifocal is better, therefore, bilateral EDOF with -0.5 to -0.75D micromonovision strategy or a mix-and-match strategy with EDOF in the dominant eye together with +3.25 near add multifocal in the non-dominant eye may be used if the patient desires more near vision.
I like both the Tecnis Symfony IOL (AMO, California) and the AT LARA 829MP (Carl Zeiss Meditec). Postoperatively, patients can show over minus values on both autorefractor and manifest refraction. The highest plus possible should therefore be prescribed by using a fogging technique.
Toric IOLs: When astigmatic correction is also required, toric IOLs provide a good option. Standard toric IOLs are available in the range of 1.5D to 6.0D cylinder (to correct 0.75D to 4.75DC). Higher powers are available when required. It is important to assess posterior corneal astigmatism to avoid errors in IOL calculation.
FUTURE
Preoperative decision making needs to become yet more refined in terms of extremely precise IOL power calculations in complex eyes as well as in having the ability to preoperatively simulate realistically to each patient the kind of vision they can expect postoperatively from a particular lens choice. This becomes especially important with presbyopic IOLs as these patients form the most demanding group and it would definitely help decrease chair time if they could be made precisely aware as to what to expect postoperatively.
Intraoperative and postoperative factors such as toric IOL alignment, postoperative rotation etc are other factors which need to be perfected yet more. Another problem that also needs to be further refined is postoperative IOL power adjustment and the ability to have effective dropless surgery via canalicular or punctal sustained release drug-delivery systems.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India and can be reached at dr_soosanj@hotmail.com
