Multicomponent IOL systems offer attractive option in certain scenarios
Cheryl Guttman Krader
Published: Saturday, February 1, 2020
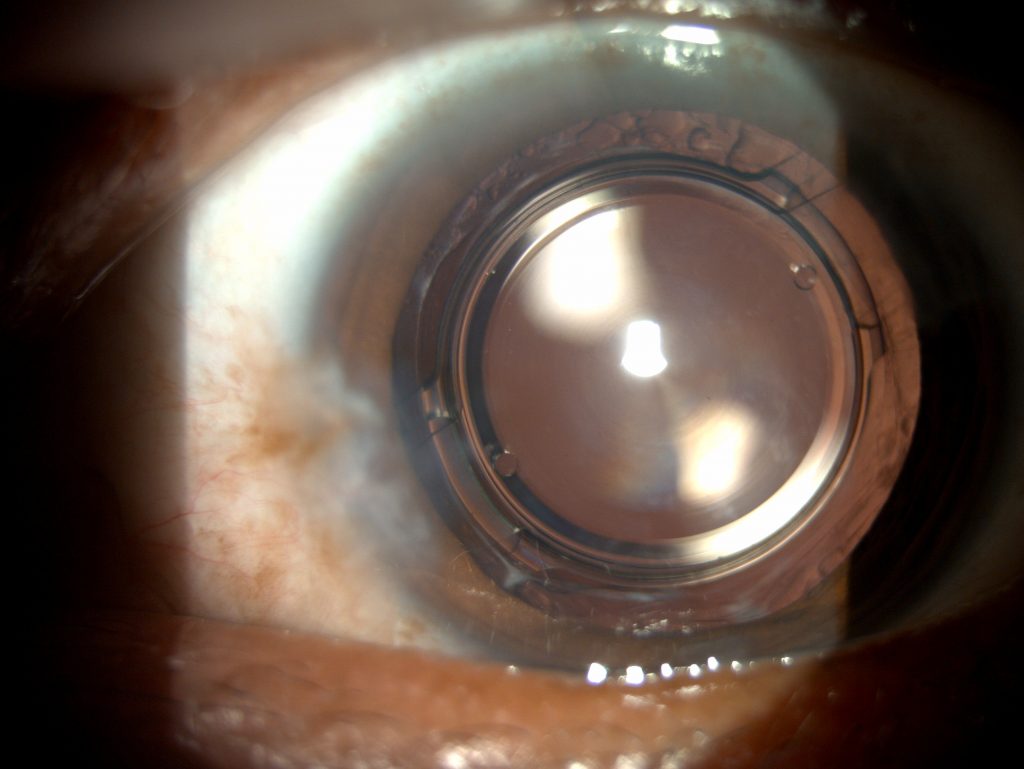
[caption id="attachment_17753" align="alignleft" width="1024"] A slit lamp photo of the Precisight with both components within the capsular bag[/caption]
Harvey S. Uy MD
Multicomponent IOLs are a safe and effective option for correcting errors of refraction and addressing multifocal IOL intolerance after cataract surgery, said Harvey S. Uy MD, at the 37th Congress of the ESCRS.
“A significant proportion of premium IOL patients are unhappy with their outcome, and a major cause for their dissatisfaction is residual refractive error. A published analysis of EUREQUO data (Lundström M, et al. J Cataract Refract Surg. 2018;44(4):447-452) showed that one-in-14 patients will have a significant refractive error of 1D or more and one-in-100 patients will have a refractive surprise of 2D or more.
These data translate into cataract surgeons having one patient with an unsatisfactory refractive outcome for every OR day,” said Dr Uy, Medical Director, Peregrine Eye and Laser Institute, Makati, Philippines.
He suggested that primary implantation of a multicomponent IOL with an exchangeable optic provides a safety net in premium IOL cases. In the future, the applications for multicomponent IOLs might also include intraocular medication delivery and blood sugar concentration detection.
Multicomponent IOLs are modular systems made of one permanent element that sits in the capsular bag and a detachable/exchangeable piece. Dr Uy has worked with two multicomponent IOLs – the Precisight (InfiniteVision Optics), which is commercially available in Europe, and the Harmoni Modular IOL System (ClarVista Medical), for which he did the first clinical study.
The Harmoni IOL consists of a donut-shaped hydrophobic acrylic base component that sits in the capsular bag and a hydrophilic acrylic optic that is attached to the centre. The Precisight IOL consists of two refractive components. The base lens is a hydrophobic acrylic lens that remains in the capsular bag permanently, while the front detachable optic is made of hydrophilic acrylic and comes in monofocal, multifocal, extended depth of focus and toric versions.
“The secondary optic has tabs that attach to the bridges on the base component and lock the lens in place,” Dr Uy said.
The primary procedure for Precisight IOL implantation is done with injection through a 2.4mm incision. The procedure for exchanging the front optic with the Precisight IOL is done through the original surgical incision and has a fairly short learning curve. It requires no additional equipment and is very safe, Dr Uy said.
“Use of the multicomponent IOL removes the time pressure that accompanies an exchange procedure for a conventional IOL. The longer we wait to exchange a conventional IOL, the more nervous we get because capsular fibrosis sets in, and so the surgery becomes more complex. With the Precisight IOL, the later you do the exchange, the easier it becomes because capsular fibrosis makes the base component more stable.” he added.
Assembly of a Precisight IOL outside of the eye
CLINICAL PROOF
Data from a study including 65 eyes implanted with the Precisight IOL demonstrate the safety and effectiveness of the exchange/enhancement procedure. The front optic was exchanged more than three months after the primary surgery in eyes with MRSE greater than 1D. Mean logMAR UDVA was 0.2 pre-enhancement and 0.0 at three and 12 months post-enhancement.
“CDVA was unchanged after the exchange procedure, and the endothelial cell count was stable too, which demonstrates the safety of the exchange,” Dr Uy said.
Mean manifest refraction spherical equivalent (MRSE) was 1.3D pre-enhancement and 0.0D at three and 12 months post-enhancement. At one year post-enhancement, MRSE was within 0.25D of target in 79% of eyes, ±0.50D in 92%, and ±1.0D in all cases.
“The IOL position is stable after the enhancement. The data in this series show that the exchange procedure is associated with very robust correction of refractive error and good refractive stability,” Dr Uy said.
Harvey S. Uy: harveyuy@yahoo.com

 A slit lamp photo of the Precisight with both components within the capsular bag[/caption]
A slit lamp photo of the Precisight with both components within the capsular bag[/caption]
 Harvey S. Uy MD
Harvey S. Uy MD Assembly of a Precisight IOL outside of the eye
Assembly of a Precisight IOL outside of the eye