Cornea
Knowing Iris Repair: Pupilloplasty
This second of the series on iris repair covers everything pupilloplasty.
Soosan Jacob
Published: Friday, March 1, 2024
Pupilloplasty can be done for visual purposes to decrease glare or reduce the effect of HOAs, for anatomical reasons to create a taut iris diaphragm and prevent peripheral anterior synechiae, or for aesthetic reasons, e.g., to correct an ectopic pupil or close an iris defect in light-coloured irides.
Iris reconstruction should therefore be an essential skill for all anterior segment surgeons. In the second of this multi-part series on iris repair, we will discuss various pupilloplasty techniques, some which can also be used for haptic fixation to the iris.
Most iris reconstruction techniques use a 10-0 or 9-0 prolene suture on a long, thin, and curved CI-4 needle, though a long and straight needle may also be used if curved is unavailable. Pupilloplasty is difficult in phakic eyes for fear of damage to the crystalline lens from the needle passes and are also not preferred because of the difficulty during a subsequent cataract extraction. Thus, if pupilloplasty is required, it is preferable to do a cataract surgery and implant the IOL first.
McCannel suture
Introduced in 1976, the McCannel suture technique uses a 10-0 prolene suture on a long needle introduced through the limbus and passed through the approximated first and second iris edges and out the limbus on the other side. The suture on either side of the iris is then retrieved with a Sinskey or Kuglen hook passed through a paracentesis created between the two limbal sites and a single or double knot is slowly and gently tightened to approximate the iris edges. Further knots are then thrown. The McCannel suture has the disadvantage of traction on the iris towards the paracentesis while tightening the knots that may not be tight enough.
Siepser sliding knot
Siepser modified the McCannel suture in 1994 by introducing the sliding knot to make tightening easier and less traumatic to the iris. It gives a tighter knot and better approximation of the iris. Here, the knot is tied outside the eye and then drawn in to be tightened over the iris.
A long, thin, curved needle on a 10-0 prolene suture is passed from the limbus through the first and second limbs of the iris and then railroaded into a 26-gauge needle passed into the anterior chamber (AC) through a limbal paracentesis and thus brought out. A Sinskey or Kuglen hook is passed through the paracentesis and the initial length of the suture before the first pass through the iris is hooked and brought out through the paracentesis in the form of a loop. The trailing segment is then passed over and under one side of the retrieved loop to create the knot.
Osher’s modification
Professor Robert Osher’s modification of the Siepser knot created two consecutive slip knots around a carefully untwisted, retrieved suture loop—the first one tightened after passing the cut end twice around the strand emanating from the iris, followed by retrieval of the loop again to create one locking knot.
Condon’s modification
Dr Garry Condon modified the Siepser knot by using forceps to wrap one side of the loop around the suture, just as in a simple double throw knot.
Single-pass, four-throw pupilloplasty
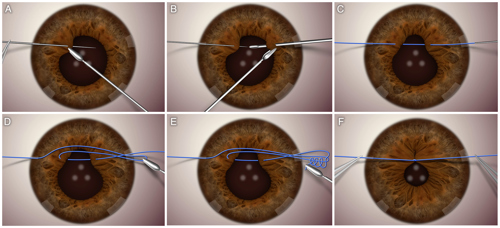
Dr Amar Agarwal modified this further by using only a single pass and four throws. A paracentesis is created at the site through which the needle will emerge after the second iris pass. Any pre-existing paracentesis sufficiently close may also be used instead.
The first limb of the iris to appose is held with a microforceps that passes through this paracentesis. A 10-0 prolene suture on a long, thin, curved CIF-4 needle or a straight STC-6 needle is passed trans-limbally through the iris root, sufficiently close to the edge to prevent undue iris bunching but with sufficient gap to prevent cheese-wiring. The needle is then carefully released and allowed to rest freely. Followed by a 30-gauge needle passed through the paracentesis, taking care not to engage corneal tissue.
The second limb of the iris is held firmly by a microforceps passed through a second paracentesis, and the 30-gauge needle is passed through the iris, again close to its edge. The needle on the 10-0 prolene suture is docked into this 30-gauge needle and railroaded out through the paracentesis. A Kuglen or Sinskey hook draws a loop of the initial pass of the suture out through the paracentesis. The free end of the suture is then cut and looped four times around the externalized loop. The two ends of the suture on either side of the limbus are then pulled in opposite directions—this internalizes the knot and tightens it over the iris, bringing the two limbs of the iris together. Advantages include ease of surgery and the ability to use either limb of the externalized loop.
Pinhole pupilloplasty (PPP)
As described by Dr Agarwal, the pupil is made pinhole sized to remove the effect of HOAs and improve visual acuity in eyes with high amounts of irregular astigmatism.
Open-sky pupilloplasty
A pupilloplasty is often needed in combination with a penetrating keratoplasty. In this case, an open-sky pupilloplasty may easily be done. A short, curved needle on a 10-0 nylon suture is often easier to pass than the long, curved needle attached to the 10-0 prolene suture. Care should be taken to avoid excess pulling to avoid any tug on the ciliary body in the open-sky state.
Complications
There must be enough stretch in the iris to bring the limbs together from either side. If pulled without sufficient laxity for the two limbs to appose, the suture can cheese-wire through the iris, or the iris can detach from its root, creating an iridodialysis and bleeding into the AC. Excessive stretch can also result in iris stromal tears, iris hole creation, etc. Extensive manipulation can result in postoperative iritis.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
Latest Articles
Towards a Unified IOL Classification
The new IOL functional classification needs a strong and unified effort from surgeons, societies, and industry.
Organising for Success
Professional and personal goals drive practice ownership and operational choices.
Update on Astigmatism Analysis
Is Frugal Innovation Possible in Ophthalmology?
Improving access through financially and environmentally sustainable innovation.
iNovation Innovators Den Boosts Eye Care Pioneers
New ideas and industry, colleague, and funding contacts among the benefits.
José Güell: Trends in Cornea Treatment
Endothelial damage, cellular treatments, human tissue, and infections are key concerns on the horizon.
Making IOLs a More Personal Choice
Surgeons may prefer some IOLs for their patients, but what about for themselves?
Need to Know: Higher-Order Aberrations and Polynomials
This first instalment in a tutorial series will discuss more on the measurement and clinical implications of HOAs.
Never Go In Blind
Novel ophthalmic block simulator promises higher rates of confidence and competence in trainees.